






Posterior vitreous detachment (PVD) is a natural age-related change in your eye, typically occurring around 40-50 years of age, and can lead to visual disturbances such as 'floaters', flashes of light, and shadows in the visual field. Often it is harmless and requires no treatment, but in some cases, it can be very bothersome. Read on to learn about what posterior vitreous detachment is and when it may be necessary to seek help.
What is posterior vitreous detachment?
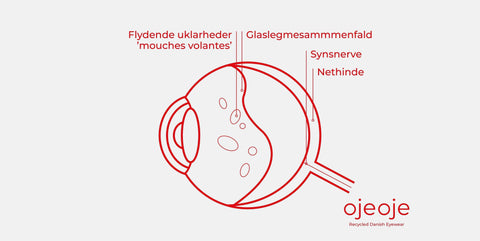
Posterior vitreous detachment, also called vitreous separation, is a natural change in your eye that occurs with age when the vitreous humor slowly becomes less firm and collapses. This change causes the vitreous humor to pull away from the retina, breaking the weak attachment to the retina at the back of the eye. This process is called posterior vitreous detachment and can lead to visual disturbances such as flashes of light, moving opacities, also known as mouches volantes (floaters), shadows, and dark spots in the visual field. Although it is often harmless and requires no treatment, in some cases it can be bothersome or lead to complications such as retinal detachment, which requires immediate treatment.
Why does posterior vitreous detachment occur?
The vitreous humor is a firm gel ball that fills your eye and is firmly attached to the retina. As we age, the collagen fibers in the vitreous humor begin to clump together, and the firm structure turns into a liquid mass. This process causes the vitreous humor to gradually shrink and collapse. The detachment causes the vitreous humor to pull away from the retina, which can cause disturbances in your visual field. When the vitreous humor pulls away from your retina, it can create traction on the retinal surface. This can trigger flashes of light, as the photoreceptor cells in the retina react to the mechanical stimulation. The moving opacities feel like 'flying flies' (floaters) and occur when small collagen fibers or remnants of the vitreous humor float around in the liquid vitreous and cast shadows on the retina.
Who gets posterior vitreous detachment?
The vast majority of people will experience posterior vitreous detachment in their lifetime, with symptoms such as mobile opacities in the vitreous humor appearing from age 40-50. In addition to natural aging, other factors can also increase the risk of PVD occurring earlier or more suddenly. People with high myopia often have a longer eye, which can alter the structure of the vitreous and cause it to shrink faster and detach earlier than in people with normal vision. Eye injuries, eye surgeries, or diabetes can also accelerate the process.
What does posterior vitreous detachment feel like?
Symptoms of posterior vitreous detachment can vary from person to person, but you will often notice visual disturbances such as:
• Floating opacities in the visual field are the most common symptom. You may experience a spot or a line that moves when you change your gaze. It can also feel as if flies are flying past your eye – also known as mouches volantes. These opacities do not disappear, but you will usually get used to them over time.
• Flashes of light like lightning or strobe lights are another symptom. The flashes are often seen to the side of the visual field and last a few seconds.
These symptoms are caused by the vitreous humor detaching from the retina, which can cast shadows on the visual field. Floating opacities move when you move your eyes and can be most visible when you look at something bright, such as a white wall or a lit screen. Flashes of light occur when the vitreous humor pulls on the retina, stimulating the light-sensitive cells in the eye. For some people, the symptoms can be very bothersome at first, but they subside over time as the brain gets used to them and filters them out of the visual input. If you experience worsening symptoms such as more flashes of light, significantly more floaters, or sudden decreased vision, you should immediately seek an ophthalmologist, as this could be a sign of a more serious condition such as retinal detachment.
What is retinal detachment (amotio retinae)?
When the vitreous humor shrinks and collapses, it pulls away from the surface of the retina. If the bond to the retina is very strong, the traction on the retinal surface will cause symptoms of flashes of light. If the traction continues, it can cause the retina to tear, creating retinal tears that can develop into retinal detachment. Retinal detachment is a serious condition and, in the worst case, can result in vision loss. Therefore, it is important to seek medical attention if retinal detachment is suspected.
How long does posterior vitreous detachment last?
As a general rule, posterior vitreous detachment does not require treatment and will usually resolve on its own after a few months. However, this can vary from person to person and depends on how quickly the vitreous humor detaches from the retina, as well as how your body reacts to the detachment. But typically, it will take most people from a few months to a year to get used to the changes and symptoms that occur with posterior vitreous detachment. Discover the 3 phases of posterior vitreous detachment:
1. Initial phase (0-3 months):
In the first few months, symptoms such as flashes of light and floating opacities resembling 'flying flies' (mouches volantes) or 'flying streaks' and dots may be what you notice as the vitreous detaches from the retina. Many will find that the floating opacities are more visible against a bright wall.
2. Adaptation phase (3-6 months):
After the initial period, your brain begins to adapt to the new visual impressions. Many experience that the symptoms slowly diminish as there are fewer floating opacities, or they are filtered out by the brain. Flashes of light may still occur, but they also decrease and become less intense.
3. Long-term phase (6-12 months):
Most people will notice their vision stabilizing over time. Floating opacities become less visible, or they 'freeze' in a specific spot in the visual field, making them less irritating. In many cases, only a few continue to experience problems after a year.
How do you know if you have posterior vitreous detachment?
An ophthalmologist can diagnose posterior vitreous detachment with a thorough eye examination, where the inside of the eye is examined using a slit lamp and an ophthalmoscope. In some cases, ultrasound is used to rule out complications.
Can you have surgery for posterior vitreous detachment?
In most cases, posterior vitreous detachment requires no treatment, as the symptoms will subside over time. However, if the symptoms are very bothersome and affect your daily life, surgical treatment such as vitrectomy (surgical removal of the vitreous) or laser treatment (YAG laser vitreolysis) may be considered.
Can you see without vitreous humor?
The vitreous humor, as previously described, is a gel ball that fills the eye and helps maintain its shape. Although the vitreous humor plays an important role in the early development of the eye, it is not essential for vision itself. When the vitreous humor is removed, it is replaced with a fluid or gas, which over time is replaced by the eye's own fluid (aqueous humor). Since the vitreous humor consists primarily of water, its removal has no direct impact on vision, as long as the retina and lens function normally.
When is posterior vitreous detachment surgery considered?
• If symptoms such as 'floaters', dots, and streaks significantly disturb your vision and affect your daily life and activities – e.g., reading, working, and driving.
• If there are persistent flashes of light or traction on the retina, which increases the risk of complications such as retinal detachment.
• If bleeding occurs in the vitreous (as in diabetic retinopathy).
Can you prevent posterior vitreous detachment?
Posterior vitreous detachment cannot be prevented, as it is an age-related condition that naturally occurs with time when you reach 40+ and for some even earlier. But there are some things you can keep in mind to maintain healthy eyes:
• Protect your eyes: Prolonged exposure to the sun's harmful ultraviolet rays is not good for your eyes. Wear sunglasses with UV protection to protect your eyes in the sun. See all our recycled sunglasses and prescription sunglasses
• Eat healthily: Foods with vitamins A, C, and E, as well as zinc and omega-3 fatty acids, are good for eye health – e.g., kale, spinach, carrots, berries, and fatty fish like salmon.
• Limit screen time: Too much screen time can cause dry and tired eyes. Remember to take breaks and blink more often to maintain moisture in your eyes.
• Get enough sleep: When you sleep, your eyes get a chance to rest and rejuvenate themselves – they recover at night.
• Eye examinations: Get regular examinations from an optician or ophthalmologist – especially if you are nearsighted or have other risk factors such as eye injuries and diabetes, which can accelerate the process.
Is posterior vitreous detachment dangerous?
Posterior vitreous detachment sounds dramatic, but in most cases, it is quite harmless. Although posterior vitreous detachment is a normal part of the body's aging, there are symptoms you should take seriously. Complications such as retinal detachment can occur, requiring prompt treatment to avoid permanent vision loss. If the vitreous pulls too much on the retina, small tears can occur, which can lead to retinal detachment. This can result in vision loss if not treated quickly. Symptoms such as increasing flashes of light, an increased number of 'floaters', or a large shadow in the visual field should always be examined by an ophthalmologist.
Posterior vitreous detachment and time for reading glasses – are they related?
Yes – posterior vitreous detachment and the need for reading glasses are related, but not because one directly causes the other. They often occur at the same time in life – typically around 40-50 years of age. This is no coincidence. With age, your lens becomes less flexible. This makes it harder for you to focus on text and nearby objects (presbyopia) – and that's why you suddenly need reading glasses, even if you may have had perfect vision your whole life. Discover our wide selection of recycled reading glasses.
When should you seek medical attention?
Although posterior vitreous detachment is not dangerous, it is important to pay extra attention to the symptoms listed below after a confirmed posterior vitreous detachment, as in rare cases it can lead to serious complications such as retinal detachment. Retinal detachment (amotio retinae) is a serious eye condition where the retina – the thin, light-sensitive membrane at the back of the eye – detaches from the underlying layers that supply it with nutrients and oxygen. If the condition is not treated quickly, it can lead to permanent vision loss. If you experience one or more of the following symptoms that may indicate retinal detachment, you should contact your general ophthalmologist. If it is not possible to see an ophthalmologist, you should contact an emergency doctor for an urgent appointment at an eye department. Look out for 5 symptoms of retinal detachment:
• Increasing flashes of light.
• Significantly more 'floaters'.
• Blurred or distorted vision.
• Sudden decreased vision.
• A fixed grayish shadow in the visual field.
Facts about posterior vitreous detachment
• Posterior vitreous detachment often begins from age 40-50.
• Approximately 65% of people over 65 experience a posterior vitreous detachment.
• By age 80, up to 90% have had a posterior vitreous detachment in at least one eye.
• Approximately 80-90% of those examined for posterior vitreous detachment do not have retinal tears.
• Approximately 85-90% of posterior vitreous detachment cases require no treatment.
• Nearsighted (myopic) individuals may experience it earlier in life – often in their 30s-40s.
• Previous eye surgeries, e.g., for cataracts, also increase the risk.
• Most often occurs first in one eye, but the other eye typically follows within 6-24 months.
• Approximately 70-80% experience sudden 'floaters' in the visual field.
• Approximately 50% experience flashes of light – especially in dark environments.
• Symptoms (floaters and flashes) often gradually subside over weeks to months.
• The risk of complications is greatest in the first 6 weeks after symptoms appear.
• Approximately 1-3% develop retinal detachment, which requires acute treatment.

















