






Retinal detachment is a serious eye condition that can lead to permanent vision loss if not treated in time. Read on to get answers to the most relevant what, why, how, when, who, and where questions, so you know what to look out for – and what to do if symptoms appear.
What is the retina?
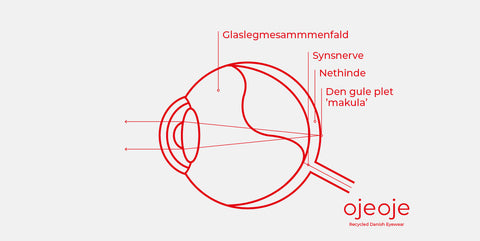
The retina is a thin layer of light-sensitive cells located at the back of the eye – like an internal film roll. This is where light enters the eye and is converted into electrical signals, which are then sent to the brain via the optic nerve. This is how you see. The retina contains millions of sensory cells that register light, colors, and movements. In the center is the macula, which provides your sharp vision. The retina is crucial for vision, and if it is damaged, it can lead to severe vision problems or, in the worst case, blindness.
What is retinal detachment?
Retinal detachment, also called 'amotio retinae', occurs when the retina separates from its normal underlying tissue. When this happens, the retina no longer receives oxygen and nutrients, which can lead to vision loss if not treated quickly. Retinal detachment often starts with small tears or holes in the retina due to posterior vitreous detachment. This allows fluid to seep in behind the retina and lift it away from the eye wall. Typical symptoms include flashes of light, sudden onset of 'floaters' (black spots or lines in your field of vision), and a dark shadow moving across the field of vision. It is important to react immediately – the sooner you are treated, the greater the chance of saving your vision.
Why do you get retinal detachment?
There are several causes and risk factors. Retinal detachment is seen in people with myopia or after eye injuries, but is often due to age-related changes in the vitreous humor – the gel-like substance that fills most of the eye. When the vitreous humor shrinks, it can tear a hole in the retina, allowing fluid to seep in behind the retina and detach it. Identify the most common causes:
• Small tears in the retina due to aging or eye injuries.
• Severe myopia which significantly increases the risk.
• Previous eye surgeries, e.g., for cataracts.
• Eye injuries, e.g., from sports or falls.
• Heredity if retinal detachment runs in your family.
• Diabetes, especially if you have diabetic retinopathy (retinal damage due to diabetes).
How do you detect retinal detachment?
The most important thing is to react to early symptoms. Retinal detachment develops quickly and painlessly, so it's easy to overlook. Typical symptoms:
• Flashes of light, especially in the dark.
• 'Floaters' (mouches volantes) which are black spots or lines in the field of vision.
• Shadow in the field of vision, often like a curtain-like shadow.
• Blurred vision or distorted vision.
• Sudden loss of vision in parts of your field of vision. – you may experience one or more of these symptoms, and they can develop over hours or days.
When should you seek help?
Immediately. If you suddenly experience flashes of light, many new black spots, or a shadow in your vision, you should contact an ophthalmologist or go to the emergency room at once. The sooner you receive treatment, the greater the chance of saving your vision. Do not wait and see, as you may lose valuable time if your retina has already detached.
Who is at risk of retinal detachment?
Although anyone can be affected, some groups are more vulnerable than others. You have a greater risk if you:
• Are over 50 years old as age-related changes increase the risk.
• Are very nearsighted, especially with prescriptions over -6.
• Have had previous eye surgery.
• Have had retinal detachment in the other eye.
• Have been exposed to eye injuries.
• Have an inherited eye disease.
– if you belong to one of these groups, you should be particularly aware of changes in your vision.
How does the ophthalmologist diagnose it?
The ophthalmologist diagnoses retinal detachment by first asking about your symptoms such as flashes of light, 'floaters', or blurred vision. Your eye is then examined with specialized equipment, typically after the pupil has been dilated with eye drops. With an ophthalmoscope or a slit lamp with a lens, the doctor can see if the retina has detached. If there is bleeding or opacities, an ultrasound scan may be supplemented. The diagnosis is based on the examination and your symptoms, and if retinal detachment is suspected, you will be referred for treatment quickly. The examination is painless, but it may take some time – especially if your pupils need to be dilated.
How is retinal detachment treated?
The treatment of retinal detachment depends on the severity of the detachment and its location. In most cases, surgery is required and must be performed quickly to save vision. The most common method is vitrectomy, where the ophthalmologist removes the vitreous humor and replaces it with gas or oil to push the retina back into place. In some cases, laser or cryotherapy is supplemented to close holes in the retina.
After the operation, you must keep your head in a specific position for a few days so that the gas presses in the correct place. Vision gradually returns over weeks to months, and the result depends especially on whether the macula has been affected. The macula is the area in the center of the retina that allows you to see sharply and read details. If the retinal detachment reaches the macula, there is a greater risk of permanent vision loss.
What are your chances of regaining your sight?
It depends primarily on whether the macula is involved. If the macula is not detached, you have up to a 90-95% chance of regaining almost full vision. If the macula is detached, you may only have a 50% chance of good vision again, and it rarely returns to completely normal. The sooner you receive treatment, the better your chances.
How do you prevent retinal detachment?
You cannot always prevent it, but you can do a lot to reduce the risk and react in time. This is especially about knowing your symptoms and getting regular eye exams – especially if you are nearsighted or have had previous eye surgery. Seek an ophthalmologist immediately if you experience visual disturbances such as flashes of light, black spots and lines, or a shadow in your field of vision. Prompt action can make the difference between preserved and lost vision. Get the best advice:
• Get regular eye exams, especially if you are nearsighted or over 50.
• Be aware of changes in your vision and react quickly.
• Protect your eyes during sports and gardening with sunglasses or glasses without prescription if there is a risk of impact.
• Get retinal tears treated early, before they become detachments.
• Keep your diabetes under good control, if you have it.
Retinal detachment and time for reading glasses – is there a connection?
Not directly, but there is an indirect connection. When you reach your 40s and start needing reading glasses, it is due to age-related farsightedness (presbyopia), where the eye's lens loses its ability to focus on close objects. This in itself does not increase the risk of retinal detachment, but in the same age group, the vitreous humor (the gel that fills your eye) begins to change and detach from the retina. This is called age-related posterior vitreous detachment, and it happens to almost everyone over time. In some, it can tear a hole in the retina, which can lead to retinal detachment.
Short questions/answers:
What is retinal detachment?
A detached retina in the eye that can lead to permanent vision loss.
Why does it occur?
Retinal tears, nearsightedness, age, trauma, illness.
How do you detect it?
Flashes of light, black spots and lines, shadow vision, and reduced vision.
When should you react?
Immediately – it is an acute condition.
Who is affected?
Mostly people over 50, nearsighted individuals, and those with eye injuries and diabetes.
Where is it treated?
In ophthalmic surgery departments and hospitals.
Ea's experience with retinal detachment
"I just thought it was old age – but then the shadow started to grow"
• Name: Ea, 57 years old
• Background: lawyer, nearsighted (-6 in both eyes)
At first, I had problems with 'floaters' – black dots dancing around, especially when I looked at a lit screen. I didn't think much of it, as I'd heard it came with age. But one Sunday morning, I woke up and experienced a strange flicker in my left eye. It seemed like a lightning flash at the edge of my visual field, appearing every time I moved my eye quickly from side to side. It wasn't uncomfortable, but it didn't seem normal. A couple of days later, on my way home from work, I saw a shadow in the lower part of my visual field – it looked like a dark curtain, half-drawn over my eye. The shadow didn't move, but it grew a little during the evening. I called my ophthalmologist the next morning and described my symptoms, and they asked me to come in immediately.
"You need surgery as soon as possible"
At the ophthalmologist's office, my eye was dilated with drops. This allowed the doctor to see all the way to the retina. He used a strong light and a special apparatus – and after a few minutes, he unfortunately confirmed that it was a retinal detachment. I had to have surgery the same day. I was scared. I had never had general anesthesia before, and the thought of someone operating on my eye was terrifying. But the doctor calmly explained that the sooner I had the surgery, the greater the chance of regaining my vision.
The surgery and the first few days after
I was sent to the ophthalmology department at Rigshospitalet, where an eye surgeon confirmed that I had retinal detachment. The surgery was performed the same evening – a vitrectomy, where they removed the vitreous humor and replaced it with a gas bubble to hold the retina in place. After the surgery, it was important to keep my head down for the first few days so that the gas would press in the correct place in the eye. It was tough and required patience, especially because I wasn't allowed to sleep on my back. Vision in the operated eye was very blurry for the first few weeks – like looking through a dirty window.
How is it going today?
Today, almost a year later, my vision in my left eye is almost normal. I have some slight blurriness at the edges, and I still have some 'floaters', but it's nothing compared to what could have happened to my vision. I've learned that I should never ignore changes in my vision. If I had waited a few more days, it might have been too late. Now I get my other eye checked regularly, and I've become better at listening to my eyes.
Ea's advice to you:
• Take changes in your vision seriously and react quickly.
• Don't wait to seek help – it can be an emergency.
• Follow the ophthalmologist's instructions carefully after surgery.
• Get regular eye exams.
• Take care of your eyes – listen to them.

















